
Despite significant advances in clinical research, there remains a staggering 17- to 20-year gap between the introduction of clinical innovations and their widespread implementation, with less than 50% of these innovations ever becoming part of routine practice.1 This delay not only hampers the potential benefits to patient care but also undermines the investment made in medical research.
Several factors contribute to the slow adoption of clinical innovations. Historically,the pace of biomedical research has outstripped society's capacity to absorb and implement new findings. Contextual factors, such as social, organisational,and policy contexts, also play significant roles.1 Financial limitations and budget constraints within healthcare systems often slow the adoption process and can impede adoption of new technologies due to significant upfront costs, even when long-term savings are evident .1 Regulatory requirements and policy frameworks further delay clinical innovations.Navigating these complex systems can be challenging, and policy changes are typically slow. Many healthcare settings also lack the necessary infrastructure, such as technology, staffing, or support systems, to effectively implement new treatments. Finally, educating and training healthcare providers in new innovations poses a significant barrier.Traditional education methods may not suffice, and reluctance to change established practices can cause delays. However, education providers can address these challenges by leveraging innovative methods to create dynamic programmes that accelerate the adoption of clinical innovations.
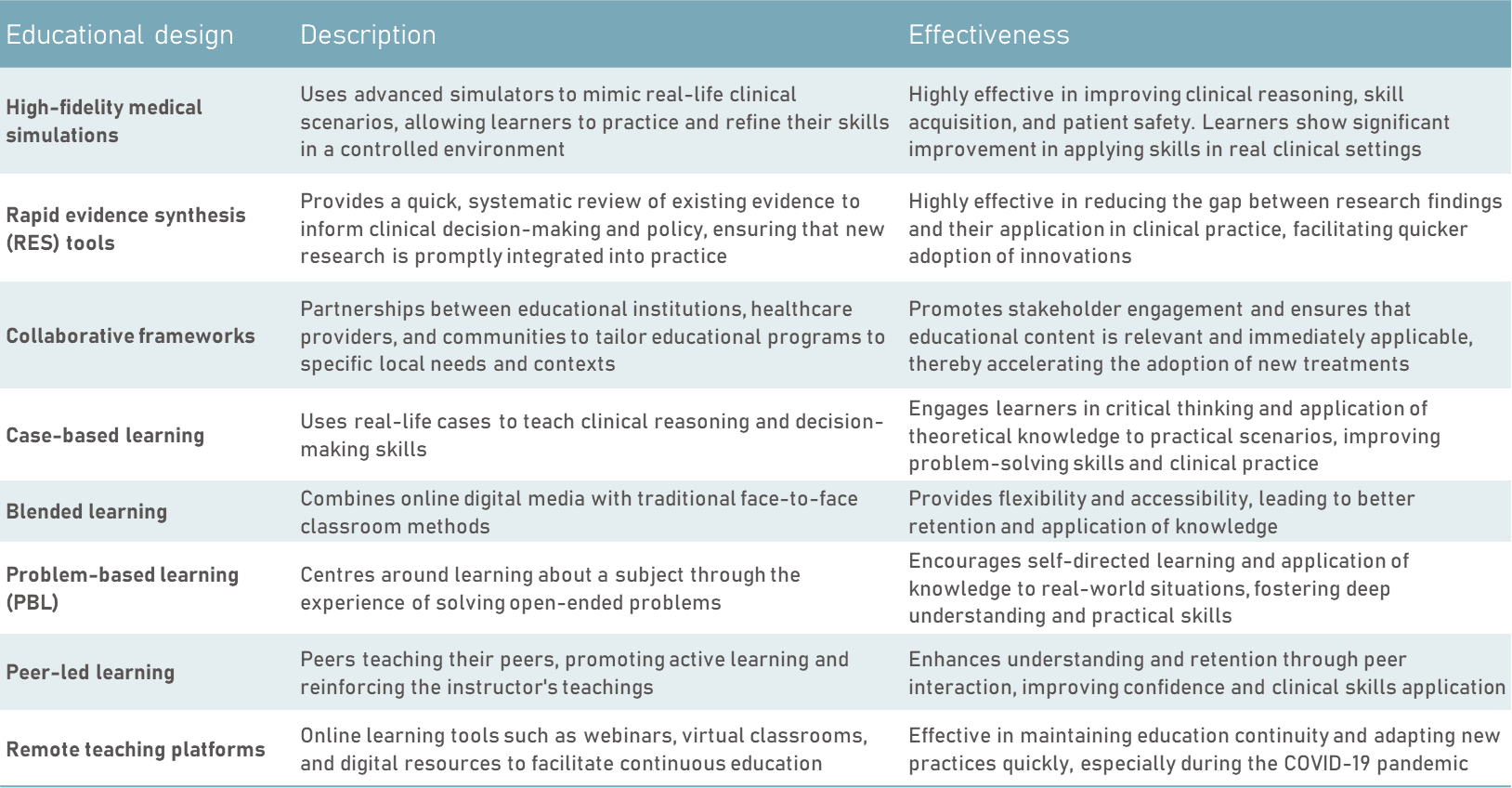
It is imperative that education providers develop programmes that offer clear,actionable skills that are easily applicable in clinical practice. By utilising novel educational design, such as high-fidelity medical simulations, remote teaching platforms, collaborative frameworks, and rapid evidence synthesis tools, learners can study a skill one day and apply it in practice the next. This generates “actionable knowledge”, which aids accelerated clinical practice adoption to improve patient outcomes.
TABLE. Summary of Educational Design Methods
References
1. Bauer, M. S., & Kirchner, J. (2019). Implementation science: What is itand why should I care? PsychiatryResearch, 283, 112376. https://doi.org/10.1016/j.psychres.2019.04.025
2. Issenberg,S. B., McGaghie, W. C., Petrusa, E. R., Gordon, D. L., & Scalese, R. J.(2005). Features anduses of high-fidelity medical simulations that lead to effective learning: ABEME systematic review. Medical Teacher, 27(1), 10–28. https://doi.org/10.1080/01421590500046925
3. Poots, A. J., Devlin, A. M.,Rudge, G., & Adler, M. (2022). Rapid evidence synthesis to enableinnovation and adoption in health and social care. Systematic Reviews, 11(1),109. https://doi.org/10.1186/s13643-022-02106-z
4. Worley, P., & Kitto, S.(2017). Using a framework to implement large-scale innovation in medicaleducation with the intent of achieving sustainability. BMC Medical Education,17(1), 18. https://doi.org/10.1186/s12909-017-0857-7
5. Thistlethwaite, J. E., et al.(2012). The effectiveness of case-based learning in health professionaleducation. A BEME systematic review: BEME Guide No. 23. Medical Teacher, 34(6),e421-e444. https://doi.org/10.3109/0142159X.2012.680939
6. Means, B., et al. (2013). Theeffectiveness of online and blended learning: A meta-analysis of the empiricalliterature. Teachers College Record, 115(3), 1-47. https://doi.org/10.1177/016146811311500307
7. Hung, W., et al. (2008).Problem-based learning: A learning environment for enhancing learning transfer.New Directions for Adult and Continuing Education, 2008(118), 21-29. https://doi.org/10.1002/ace.20042
8. Secomb, J. (2008). A systematicreview of peer teaching and learning in clinical education. Journal of ClinicalNursing, 17(6), 703-716. https://doi.org/10.1111/j.1365-2702.2007.01954.x
9. Kameg,K., Kaufmann, J., Cline, T., & Kameg, B. (2022). Incorporation of child &adolescent mental health standardized patient simulations to provideinterprofessional education for graduate students. Issues in Mental HealthNursing. 43(9), 818-823. https://doi.org/10.1080/01612840.2022.2072031